SPPM Annual Meeting - Award Winning Abstracts
Reducing Early Epidural Dislodgement with Standardized Securement
Leah Webb, MD; Alan Bielsky, MD; Kim Strupp, MD
(Submitted by Leah Webb, MD)
Department of Anesthesiology, Division of Pediatric Anesthesiology, Children’s Hospital Colorado, University of Colorado, Anschutz Campus, Aurora, CO
Early dislodgement is a key factor in the failure of epidural analgesia.1 The Pediatric Regional Anesthesia Network (PRAN) found an 18% complication rate with neuraxial catheters, with dislodgement being one of the main complications reported.2 In pediatric patients, an epidural that dislodges early is rarely replaced. Early epidural dislodgement is a preventable problem in pediatric patients that is modifiable through quality improvement initiatives.
Initially, we analyzed dislodgment rates at baseline and assessed anesthesiologists’ securement practices for epidural catheters. Out of 142 catheters, complications occurred in 13.4%, with early dislodgements occurring in 5.6%. We reviewed the literature and analyzed our data in order to identify a “best practice” for epidural securement. Numerous prior studies have compared securement techniques—such as tunneling or the use of specific devices—with conflicting and inconclusive evidence on a superior technique. Based on our data trends for securement methods, we developed a consensus on a standardized method for epidural securement. We implemented this “standardized securement method” (SSM) with the goal of decreasing our dislodgement rate by 25%.
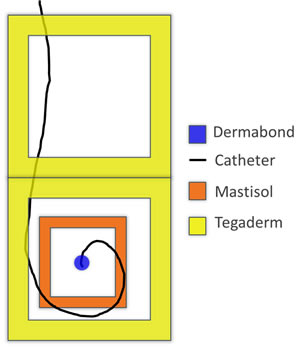 |
Figure 1. Diagram showing standardized securement method with Dermabond (R) at skin site, Mastisol (R) to surrounding area, single loop in catheter, and Tegaderm (R) covering the site and catheter. |
After collection and analysis of our baseline data, we focused on education of our faculty and trainees who would be placing and securing epidural catheters. Our securement method, diagrammed in Figure 1, involved Dermabond® at the skin site with Mastisol® Liquid Adhesive applied to the surrounding area, followed by one loop in the catheter and covered by clear occlusive dressings up the back. Notably, our acute pain advanced practice nurses were instrumental in helping with patient follow up, as well as with education of medical-surgical floor nurses about dressing reinforcement. Additionally, we updated our mandatory block note in the electronic medical record to include all of the components of securement, which had been tracked on paper during our baseline data collection. We tracked catheter complications and compliance with our securement method over a six-month period from January to June 2017.
During this period, there were 186 epidural catheters in patients ranging from one day to 17 years old. Analysis of patient demographics revealed 58% male and 42% female patients. Dislodgements occurred in 4 of 80 thoracic, one of 86 lumbar, and one of 18 caudal catheters for an overall dislodgement rate of 3.2%. Compared to our prior rate of 5.6%, we noted a 43% decrease in dislodgements after SSM. The overall complication rate decreased nearly 28% from 13.4% to 9.7%. The compliance rate with the SSM was 83.3% in patients with dislodged catheters, which is similar to the overall compliance of 85.5%.
In summary, we believe our project is the first to examine standardization of securement as a method for reducing epidural catheter dislodgement. In fact, by implementing a standardized securement technique we were able to decrease our dislodgement rate by nearly 43%. By reducing the primary cause of epidural failure, we were able to optimize the duration of epidural analgesia.
References:
- Motamed C, Farhat F, Rémérand F, Stéphanazzi J, Laplanche A, Jayr C. An Analysis of Postoperative Epidural Analgesia Failure by Computed Tomography Epidurography. Anesthesia & Analgesia. 2006; 103(4), 1026-1032.
- Polaner DM, Taenzer AH, Walker BJ, et al. Pediatric Regional Anesthesia Network (PRAN). Anesthesia & Analgesia. 2012;115(6):1353-1364.